
Home
When determining the timing of placement, consider:
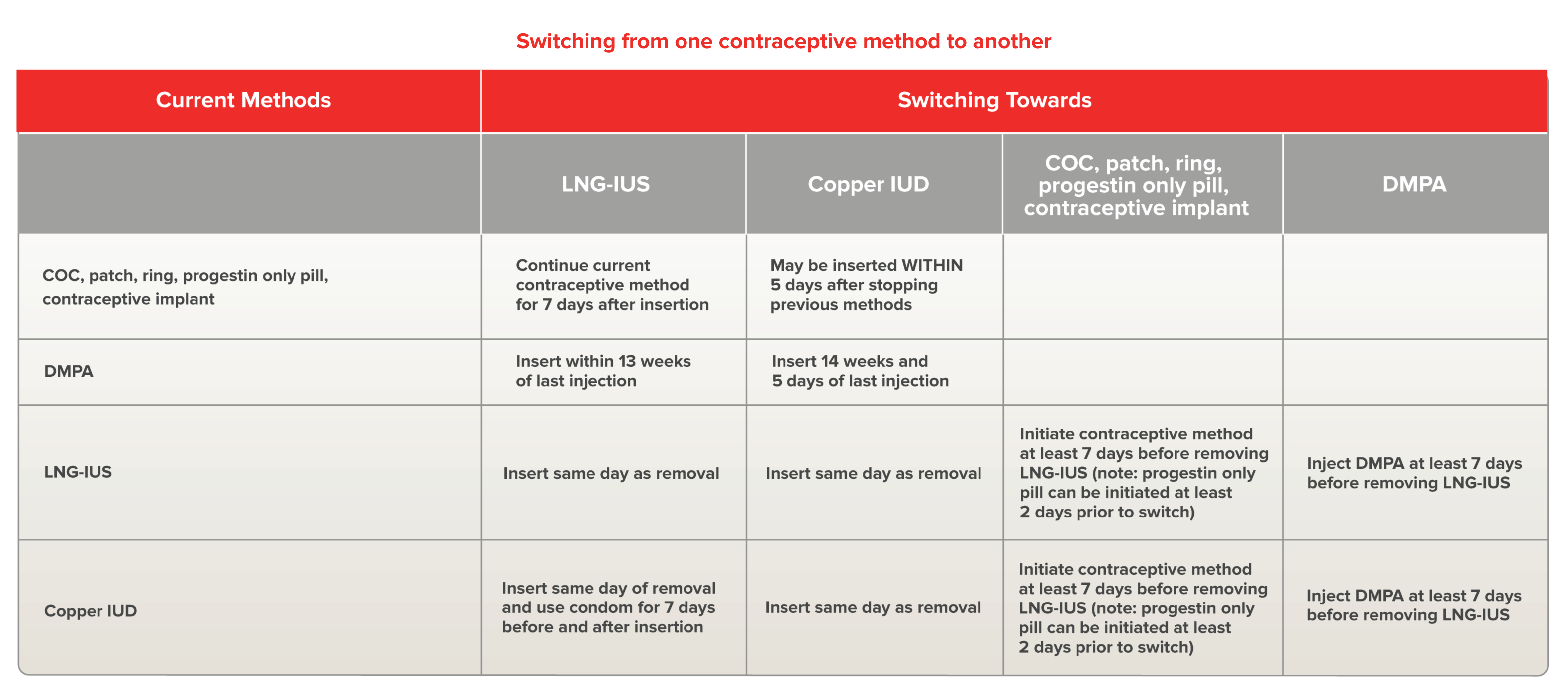
COC: combined oral contraceptives, DMPA: injectable progestin
Costescu D. and Guilbert E. et al. Preceptorship Program on
IUC insertion - Module 3
Guilbert E. et al. Addendum to the CCC- Emergency
Contraception. JOGC 2016; 38(12):1150-51.
A copper IUD can and should be used as a post-coital contraceptive:
The USAID Checklist helpful to screen a client who wants to use a copper IUD for emergency contraception.
If a woman has access to her preferred IUC, or if it has already been prescribed, the consultation and placement can take place in a single visit with a single pelvic examination in virtually all cases. A pelvic ultrasound is not required. Pelvic examination may be indicated if there is clinical suspicion of subinvolution of the uterus.
If two steps are required, the following is recommended:
Evidence suggests that IUC can be inserted immediately post-partum including during a caesarean section. Common practice has been waiting until at least 4-6 weeks post-partum, but, for maximum efficacy, IUC should be inserted within 4 weeks post-partum if a woman is not breastfeeding. Therefore earlier placement may be considered in special circumstances.Most product monographs suggest delaying until 6 weeks or involution is complete.