
Home
While cervical cancer is a contraindication to IUC placement, dysplasia is not. However, there are some special considerations related to cervical cytology and IUC use.
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception
Women switching to IUC may experience a return of acne that was present prior to the use of combined hormonal contraceptives (CHC; Pill patch or ring). If this occurs, consideration to restart CHCs should be made, or to initiate an acne therapy. In an RCT comparing copper to progestin IUC users, there was a slightly increased risk of acne among LNG-IUS users (3% vs. 5%). Women should be informed of the small risk of acne and the association with progestin-only contraception.
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception
Actinomyces forms a benign biofilm on a copper IUD in some women. Actinomyces and actinomyces-like effects may be noted on a pap, however these are not indicative of infection, and require no follow-up.
If a woman is asymptomatic, the IUC can be left in place.
If a woman develops an infection, she should be treated with penicillin G, tetracycline, or doxycycline in addition to treatment for PID.
If the infection is severe, she should be hospitalized, treated for PID with broad-spectrum coverage, and investigated for possible abscess.
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception
The Society of Obstetricians and Gynaecologists of Canada, American College of Obstetrics and Gynecology Royal College of Obstetricians and Gynecologists, and American Academy of Pediatrics all support the use of IUCs as first-line options in younger women. Additionally, the LNG-IUS is an appropriate treatment option for an adolescent who requires menstrual control or suppression.
When offering IUCs to adolescents, it may be helpful to review the following:
Black D. and Waddington A. et al. Build Your Expertise: IUC slide deck: 64-66.
In general, all hormonal contraception can be discontinued at the time of IUC placement.
Copper IUD users:
Most women who have a copper IUD placed will not require the
use of backup contraception, as the copper IUD provides both
pre-coital and post-coital (emergency) contraception in the
first cycle of use. Prior to removal, women should abstain or
use condoms for 7 days.
Progestin IUS users:
Because the LNG-IUS does not function as a postcoital
contraceptive, bridging with condoms is advisable, though
there is no conclusive data that it is necessary, and
recommendations vary from 2 to 7 days following placement.
In an observational study of cervical mucus in women with newly placed LNG-IUS, most women had poor mucus quality (i.e. unlikely to allow sperm penetration) by day 1, however 5 days were required until all women had poor sperm penetration tests.
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception Expert consensus (CNIC)
Bone Mineral Density is not affected by the presence of an LNG-IUS. BMD testing is not indicated solely due to IUC or IUS use, and should only be ordered based on current clinical guidelines.
If osteopenia or osteoporosis is noted in an IUC user, the device can be left alone as it is unrelated to the device or progestin content (if it is an IUS).
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception Expert consensus (CNIC)
The use of IUCs is not associated with increased breast cancer risk. Risk factors for breast cancer are complex, and include nulliparity, delayed childbearing, and lack of breastfeeding – there is no data to show a direct association with copper or progestin devices.
In a woman who has a history of breast cancer, a copper IUD can be used without restriction. If the woman has a hormone sensitive cancer, controversy exists on whether or not LNG-IUS can be used. If the woman has a progesterone receptor positive cancer, it should not be used. If she has an estrogen-receptor positive but progesterone-receptor negative cancer, an IUS can be used with counseling. She may wish to review this with her oncologist prior to initiating an IUS.
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception
While exclusive breastfeeding provides excellent contraception, fertility is rapidly restored upon weaning, and pregnancy can occur prior to return of menses. Therefore, breastfeeding women may wish to use an IUD or IUS for contraception.
Most suppression of lactation is derived from the estrogen component of combined hormonal contraceptives, and not the progestin. When feeding is established, placement of an LNG-IUS at the postpartum visit does not have an effect on breastfeeding success. In one small RCT, immediate postplacental IUS placement was associated with lower rates of breastfeeding, however rates of initiation of breastfeeding were low from the outset. For both Cu-IUD and LNG-IUS, postpartum state after 28 days and breastfeeding is a MEC – 1 (no contraindications).
If a woman is experiencing difficulty establishing breastfeeding, consider delaying IUS placement.
Perforation is increased when placement occurs in a breastfeeding woman. The relative risk of perforation is 6.1 (CI 3.9-9.6), however the absolute risk is low, at less than 1%. Clinicians should have a high index of suspicion for perforation when placement occurs in a woman who is breastfeeding, though routine use of ultrasound is not indicated.
While risk of perforation increases among breastfeeding women, it should not preclude IUC placement.
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception Medical Eligibility Criteria for contraceptive use. A WHO family planning cornerstone. 5th Edition, 2015.
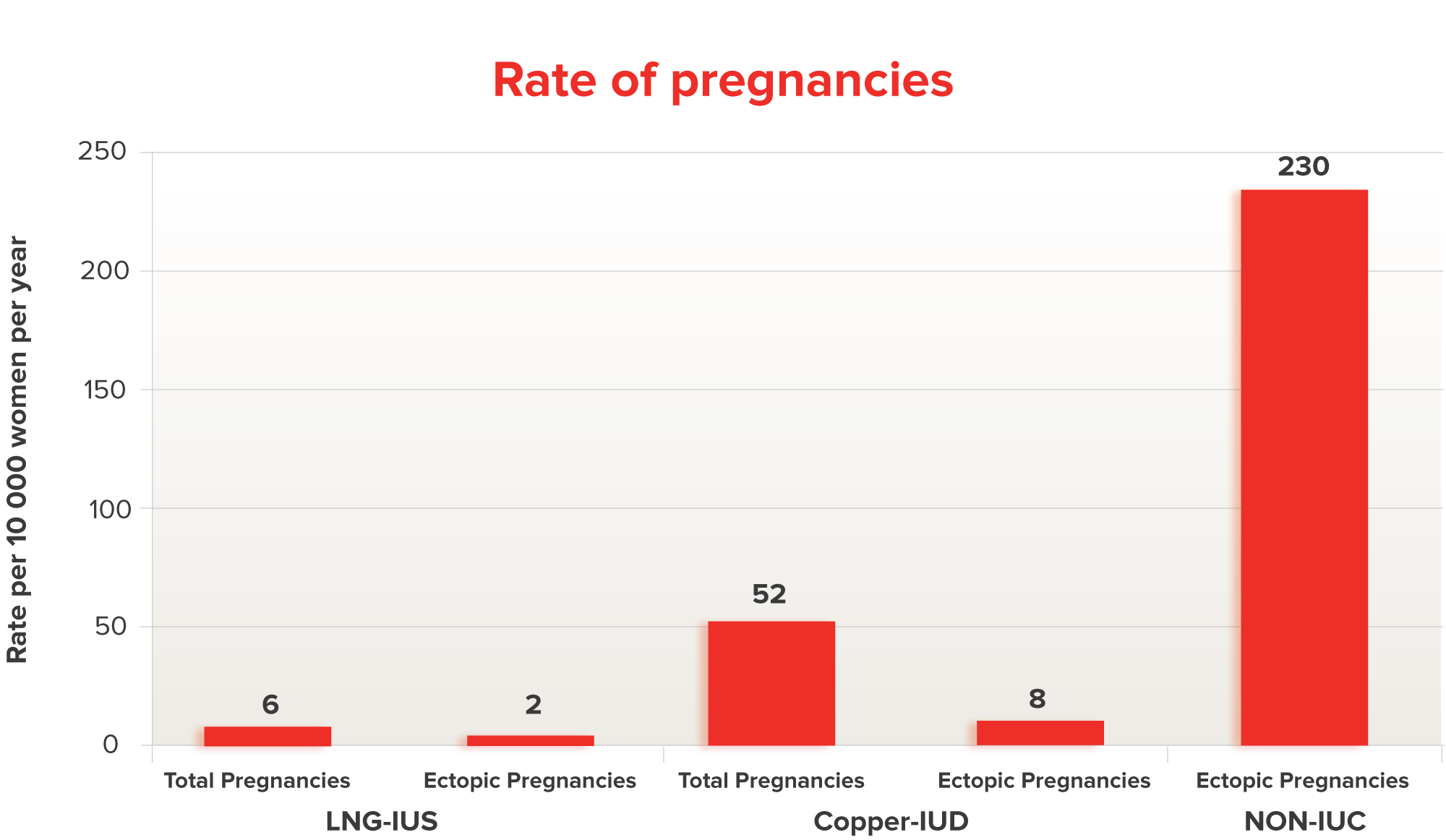
In the EURAS study of a total of 118 contraceptive failures (26 LNG, 92 copper), 21 were ectopic (7 LNG, 14 copper) resulting in incidence rates of 0.02 per 100 women per year (95% CI: 0.01-0.03) and 0.08 per 100 women per year (95% CI: 0.04-0.13), respectively. By contrast, approximately 2-3% of pregnancies in the general population are ectopic. IUCs can also be used safely by women with a previous ectopic, as the risk of pregnancy is decreased.
Pregnancies with IUC use are rare, however, when a woman becomes pregnant with IUC in place, the relative likelihood of ectopic pregnancy is increased. In the EURAS study, 27% of pregnancies with an LNG-IUS and 15% of pregnancies with a copper IUD were ectopic. These rates are similar to the risk of ectopic pregnancy among women who conceive following tubal sterilization.
Ectopic pregnancy must always be considered among women with an IUC in place who have a positive pregnancy test.
Black D. and Waddington A. et al. Build Your Expertise: IUC slide deck: 39. Costescu D. and Guilbert E. et al. Preceptorship Program on IUC insertion - Module 4 Heinemann K et al. Risk of uterine perforation with levonorgestrel-releasing and copper intrauterine devices in the European Active Surveillance Study on Intrauterine Devices. Contraception 2015; 91(4): 274-279.
Expulsions occur at a rate of approximately 3-5% over 5 years.
Most expulsions occur within the first 3 months.
Symptoms of expulsion include: cramping, vaginal discharge,
intermenstrual or postcoital bleeding or spotting,
dyspareunia, lengthened or absent threads.
Nulliparity is NOT associated with increased risk of expulsion in most studies.
Women should be advised on how to check periodically for the presence of the IUC (by feeling for the strings):
If the IUC is visible in endocervical canal or vagina – it should be removed and not be re-inserted. However, at the time of removal, a new system can be inserted immediately.
if the IUC or strings are not visible – complete expulsion may have occurred:
Costescu D. and Guilbert E. et al. Preceptorship
Program on IUC insertion - Module 4
Black D. and Waddington A. et al. Build Your Expertise:
IUC slide deck: 32-33.
Hormonal side-effects of LNG-IUS may occur, but they tend to decrease over time. These can include:
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception

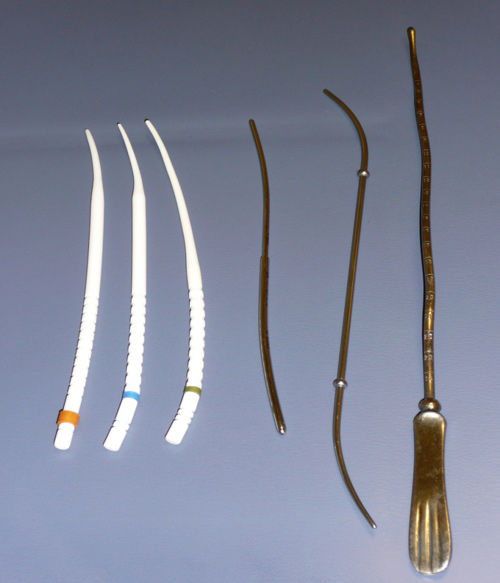


SOGC List of instruments
Costescu D. and Guilbert E. et al. Preceptorship
Program on IUC insertion - Module 3
Low libido is a complex and multifactorial condition. While libido changes are commonly reported among combined hormonal contraception (CHC, pill-patch-ring) users, it is less common among IUC users. Clinical studies show conflicting data between the use of libido changes and CHC.
If a woman experiences CHC-related libido changes, a copper IUD should be considered as a first-line treatment option, as it provides reliable contraception and is hormone free. It may take 4-6 weeks for hormonal regulation and return of libido. An LNG-IUS can also be considered among women who require menstrual management or as a second-line option. At least 6 weeks should take place with the LNG-IUS in situ before reassessing libido.
Low libido should be investigated and assessed by a specialist with clinical expertise in this area, such as a sexual medicine specialist, sexual therapist, counselor, or family physician with experience in managing sexual concerns.
Costescu et al. Levonorgestrel-Releasing Intrauterine Systems for Long-Acting Contraception: Current Perspectives, Safety, and Patient Counseling.Int J Womens Health 2016.
If an ultrasound reports a “low IUC placement”, the following steps should be considered:
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception
While there are cases of devices being accidentally removed with tampons and menstrual cups, these menstrual products can be used with an IUC in place. Because expulsion is more common in the first 3 months, it may be beneficial to avoid tampons or menstrual cups for the first 1-3 cycles following device placement, though there are no data or consensus document to dictate best practice.
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception
Some women experience a return of moliminal symptoms, such as PMS-related mood changes, when switching from combined hormonal contraception (CHC, pill patch and ring) to an IUC. Otherwise, there is no association with copper IUDs.
Mood changes (including low mood and decreased libido) are rarely reported following LNG-IUS use. These are usually self-limiting, but may require removal. Prior to removal, a discussion about pregnancy prevention is essential, as these women are at increased risk of an unintended pregnancy.
Most women with an LNG-IUS continue to ovulate, therefore IUCs are not expected to treat moliminal/PMS symptoms.
Black D. and Waddington A. et al. Build Your Expertise: IUC slide deck:39-41.
IUCs are appropriate first line options for nulliparous women
For young, nulliparous women, the need for effective long term contraception is particularly high:
SOGC Clinical Practice Guideline, Canadian Contraception
Consensus (part 3): Chapter 7 – Intrauterine Contraception
Hauck B and Costescu D. Barriers and misperceptions limiting
widespread use of intrauterine contraception among Canadian
women. J Obstet Gynaecol Can 2015;37(7):606-616.
Black D. and Waddington A. et al. Build Your Expertise:
IUC slide deck: 27,67,68.
Costescu D. and Guilbert E. et al. Preceptorship
Program – Module 3
Women who are overweight or obese are at higher risk of contraceptive failure, and may be excellent candidates for IUC, and are listed as MEC-1 (no restriction) in the US-MEC.
IUCs may be of particular benefit to overweight or obese women in the following situations:
Device placement is similar in obese women as for normal-weighted women, however the use of larger specula may make instrumentation more difficult. Use of a tenaculum is essential to improve access to the cervical os.
Medical Eligibility Criteria for contraceptive use. A WHO family planning cornerstone. 5th Edition, 2015.
In clinical trials involving the LNG-IUS, an increased incidence of ovarian cysts are noted. These are more commonly observed in the LNG-20 than the LNG-8 or LNG-12 device. In either case, these are felt to be functional ovarian cysts, likely related to LH suppression and anovulation. These cysts can be followed with ultrasound and do not usually require management. If there is clinical suspicion of an ovarian neoplasm, consultation should be obtained.
IUCs are not an effective treatment for women who experience symptomatic functional ovarian cysts, but the presence of cysts is not a contraindication to the use of either type of IUC.
Järvelä I. et al. Human Reproduction 1998;13
(2):3379-3383.
Inki P. et al. Ultrasound Obstet Gynecol 2002; 20:
381-385.
Costescu et . Levonorgestrel-Releasing Intrauterine
Systems for Long-Acting Contraception: Current Perspectives,
Safety, and Patient Counseling.Int J Womens Health
2016.
As a hormone-free contraceptive, there is no effect of a copper IUD on ovulation, although some data demonstrate that fewer oocytes are retrieved among Cu-IUD users than non-users.
In the first year of use, 76.5% of LNG-20 users were ovulating. Among LNG-12 users, 88.5% were ovulatory, and 97% of LNG-8 users were ovulatory, suggesting a dose-response.
In general, women with ovulatory dysfunction (e.g. mittelschmirz or ovarian cysts) benefit from combined hormonal contraceptives, moreso than IUC. Women using IUC should be informed that cyclical symptoms may persist, owing to ongoing ovulation.
Apter et al. Pharmacokinetics of two low-doselevonorgestrel-releasing intrauterine systems and effects on ovulation rate and cervical function: pooled analyses of phase II and III studies. Contraception 2014;101(6):1657-62.)
Cervical screening should only take place at time of IUC placement when the woman is due to be screened, based on local guidelines.
If a woman has an abnormal cervical cytology result, it should be managed as per local guidelines, regardless of whether or not an IUD is in place.
IUCs do not cause dysplasia. See Abnormal Pap Test for more information about dysplasia.
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception
When placed correctly, and when strings are left sufficiently long, a partner should not be bothered by the presence of an IUC, and dyspareunia should not occur.
If a partner is being poked or pinched by strings, they should be trimmed to be flush with the cervix. If a vertical post can be felt, examination should be undertaken on a semi-urgent basis and, if the post is visible, the device should be replaced.
If a partner notices that the strings are present, but it does not hurt, the IUC should be left alone.
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception Costescu D. and Guilbert E. et al. Preceptorship Program - Module 3
Certain clinical scenarios increase the risk of perforation. While in most cases this should not preclude an attempt at IUC placement, some clinicians will prefer to refer onwards to a more experienced provider.
Risk factors for uterine perforation:
There is insufficient evidence to show that nulliparous women are at increased risk of perforation
Symptoms of perforation at placement:
Partial perforation (uterine embedment) or complete perforation of the uterine wall or cervix may occur during or following placement. The vast majority of perforations occur at the time of placement, though it may not be detected. As such, a follow-up visit is important. A delay in detection may result in a partially perforated IUC migrating to a complete perforation (a missed opportunity to remove the IUC in the office before a complication arose). Thankfully, the risk of major complication following IUC placement, even in the setting of perforation, is very rare. Women should be informed of the small risk of perforation, and the importance of prompt diagnosis.
Most are fundal perforations and require no further management.
Costescu D. and Guilbert E. et al. Preceptorship Program on IUC insertion - Module 4
IUC’s can be placed following a first or second-trimester
surgical abortion without delay. Immediate postabortion IUC
placement is associated with decreased repeat unintended
pregnancy.
If referring a woman for abortion, consider prescribing an IUC
for same-day placement.
An IUC can be placed at the first visit following a successful
medical abortion. If there is uncertainty, an ultrasound to
confirm completion/exclude retained products, is warranted.
SOGC Clinical Practice Guideline, Canadian Contraception
Consensus (part 3): Chapter 7 – Intrauterine Contraception
SOGC - Postpartum contraception slide deck
Costescu D. and Guilbert E. et al. Preceptorship Program on
IUC insertion - Modules 2 and 4
IUCs are an excellent option for postpartum women as they provide convenient contraception and do not affect breastfeeding in women where milk supply is established.
The optimal timing of IUC placement postpartum should be individualized to the woman, her risk of unintended pregnancy, desire for contraception/fertility, and concerns about perforation. Most postpartum placements take place between 6-12 weeks, but it may be preferable to consider earlier placement (e.g. a woman who is not breastfeeding and has resumed sexual activity) or delayed placement (when the uterus has not completely involuted) at times.
In general, the longer the delay in placing an IUC, the less likely a woman is to follow-through with placement.
In a prospective study of over 60,000 women, postpartum state was associated with an increased risk of perforation,with a relative risk of 6-8. The absolute risk remains low, less than 1%. While women should be informed of this increased risk, it should not preclude women from having an IUC placed.
SOGC Clinical Practice Guideline, Canadian Contraception
Consensus (part 3): Chapter 7 – Intrauterine Contraception
SOGC - Postpartum contraception slide deck
Costescu D. and Guilbert E. et al. Preceptorship
Program on IUC insertion - Modules 2 and 4
An IUC can be placed at Caesarean Section or IMMEDIATELY
FOLLOWING DELIVERY OF THE PLACENTA
Note that the placement should be delayed if chorioamnionitis
is suspected.
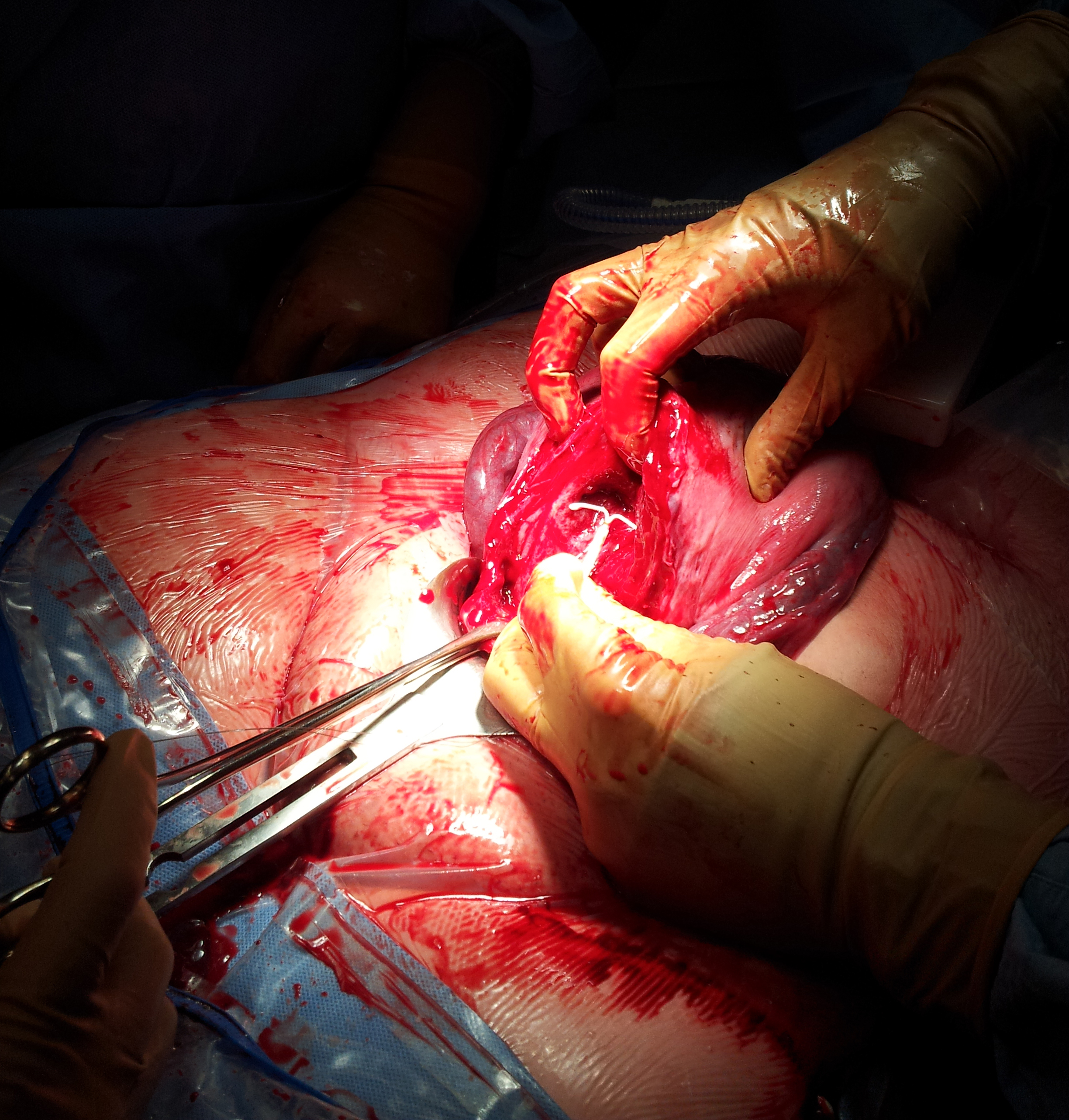 Photos from Dr.Costescu with permission
Photos from Dr.Costescu with permission
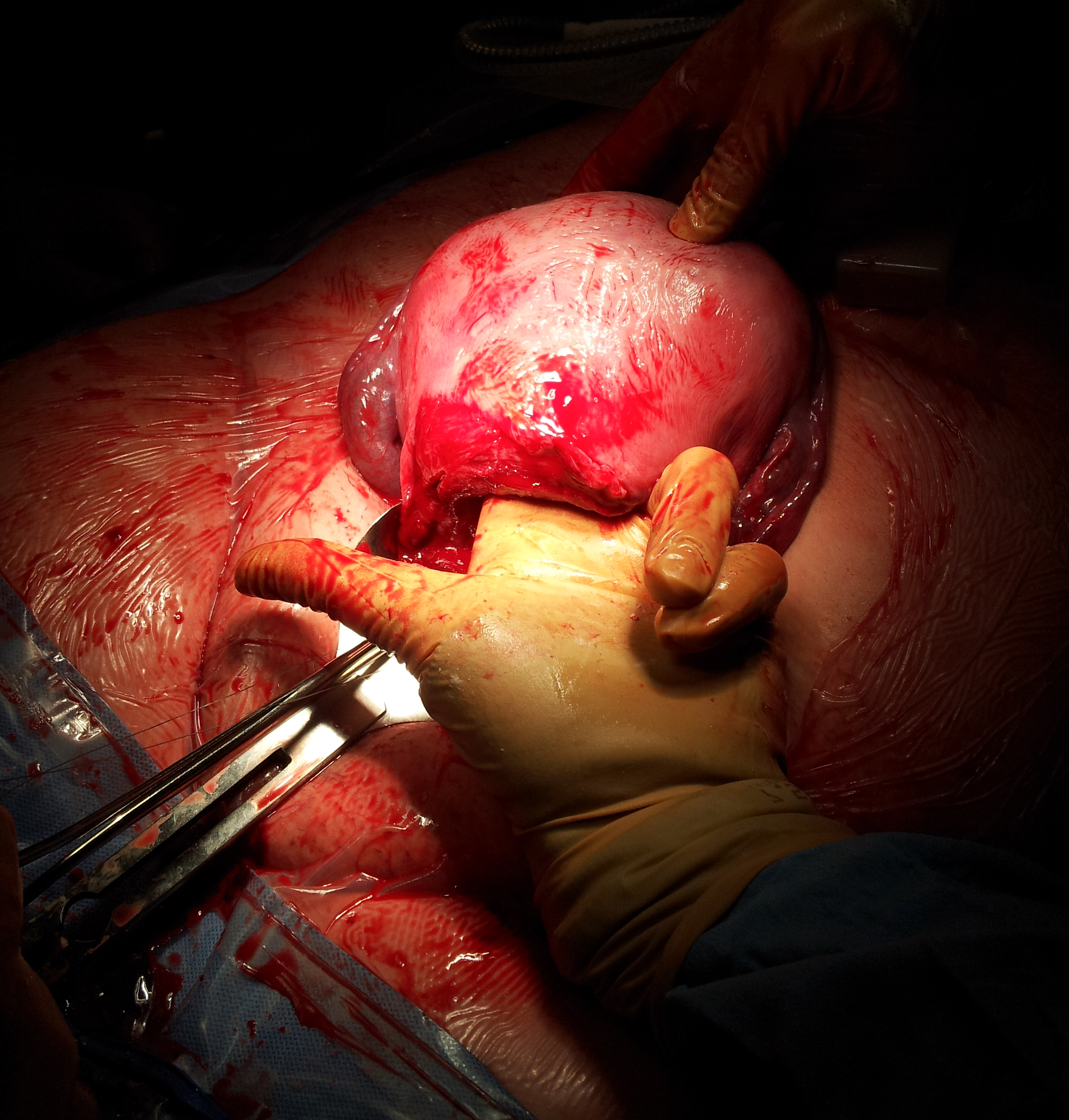 Photos from Dr.Costescu with permission
Photos from Dr.Costescu with permission
 Photos from Dr.Costescu with permission
Photos from Dr.Costescu with permission
 Photos from Dr.Costescu with permission
Photos from Dr.Costescu with permission
10 minutes after the placenta is delivered, and the uterus is assessed and found to be contracted, the device is removed from its packaging.

Immediate placement (postplacental + 10 minutes) versus Early placement (within 48 hours)
SOGC Clinical Practice Guideline, Canadian Contraception
Consensus (part 3): Chapter 7 – Intrauterine Contraception
Costescu D. and Guilbert E. et al. Preceptorship
Program on IUC insertion - Modules 2 and 4.
Costescu et al. Levonorgestrel-Releasing Intrauterine
Systems for Long-Acting Contraception: Current Perspectives,
Safety, and Patient Counseling.Int J Womens Health 2016.
A bimanual examination should be performed prior to IUC placement to assess the angle of the uterus. If there is a retroverted uterus, apply the tenaculum on the posterior lip and apply sufficient traction to correct the angle. Turning the LNG-IUS inserter upside down allows the inserter to follow a posterior path.
Costescu D. and Guilbert E. et al. Preceptorship Program - Module 4
Women and clinicians might be concerned about the impact of IUCs on fertility. Multiple studies have demonstrated rapid return to fertility following IUC removal. At 12 months following removal, 79% of CU-IUD users and 87% of LNG-IUS users were pregnant. Recall that, in the Canadian population, approximately 15% of couples will not conceive after one year of regular unprotected intercourse.
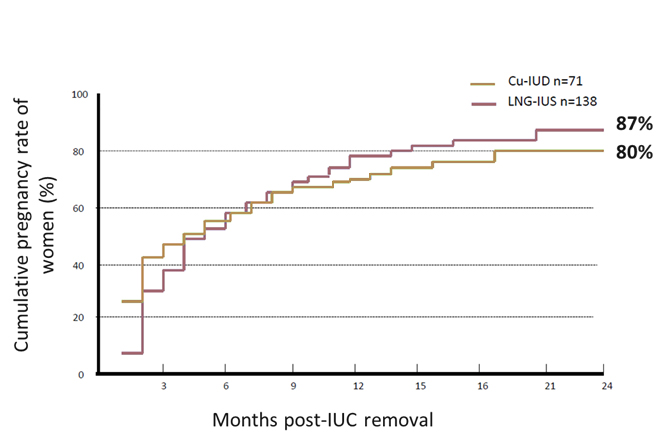
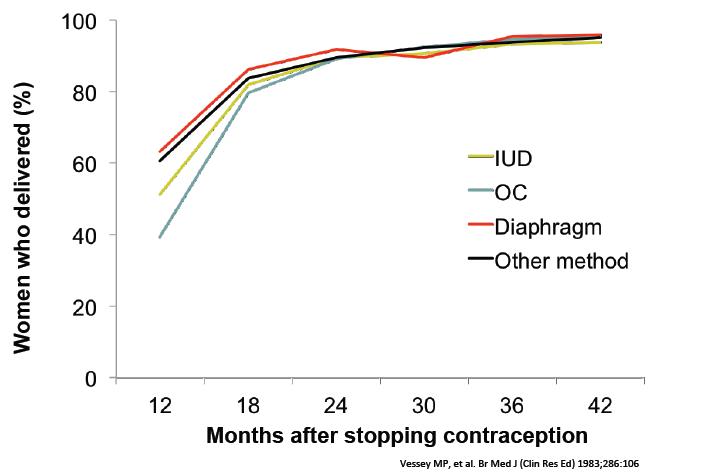
Women who are considering a family in the future will be interested in knowing how IUC will influence their future fertility. One study looking at fertility after stopping the use of an IUD showed no major differences in fertility compared to women stopping other methods (see chart below, Vessey MP. et al.).
Another randomized trial comparing the recovery of fertility after use of the LNG-20 vs. copper T380 found similar results. This trial also showed that the duration of IUC use before removal had no effect. (Belhadi H. et al.)
A recent pilot study (Stoddard et al.) also investigated the return to fertility of 111 sexually active women 18–35 years of age who had discontinued a contraceptive method and desired pregnancy. The investigation showed that pregnancy rates at 12-months were similar between former IUD users and users of other contraceptive methods (81% vs. 70%). (Stoddard et al.)
Previous studies of copper intrauterine devices (IUDs), many of which are no longer in use, suggested that they might cause tubal infertility. The concern that IUCs containing copper--currently the most commonly used type--may increase the risk of infertility in nulligravid women has limited the use of this highly effective method of birth control.
In a study examining factors associated with tubal infertility and prior IUD use, tubal infertility was not associated with the duration of IUC use, the reason for the removal of the copper IUD, or the presence or absence of gynecologic problems related to its use. The presence of antibodies to chlamydia was associated with infertility.
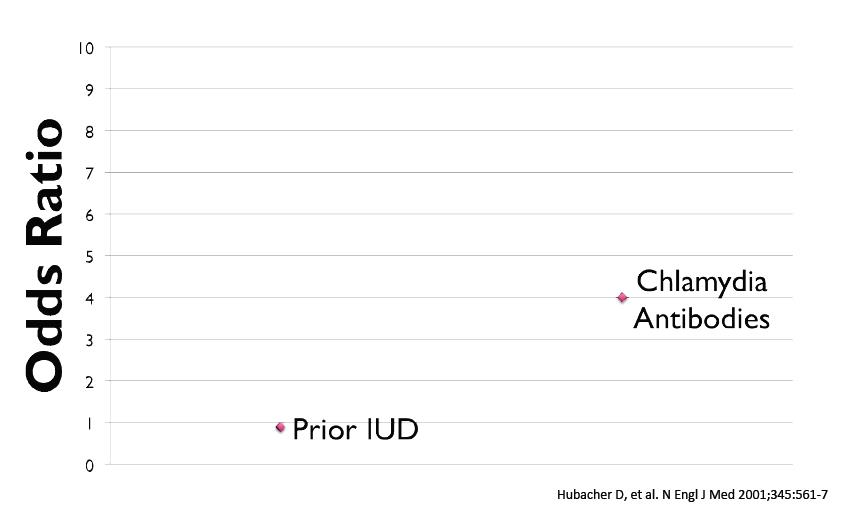
Several confounders offer reporting of risk of infertility with IUC, including: Over diagnosis of PID in copper IUD users, inability to control for sexual behaviour, choices of inappropriate comparison groups. Rates of PID following infection are similar REGARDLESS of an IUD being present.
Vessey MP et al. Fertility after stopping use of
intrauterine contraceptive device.
Br Med J (Clin Res Ed) 1983; 286:106.
Belhadi H. et al. Recovery of fertility after use of
levonorgestrel 20 mcg/d or Copper T380 Ag intrauterine device.
Contraception 1986; 34(3):261-7.
Stoddard et al. Fertility after IUD Removal: A Pilot
Study. Eur J Contracept Reprod Health Care.
2015;20(3):223-230.
Hubacher D. et al. Use of copper intrauterine devices
and the risk of tubal infertility among nulligravid women.
N Engl J Med 2001;345:561-7.
Black D. and Waddington A. et al. Build Your Expertise:
IUC slide deck: 25-26.
Costescu D. and Guilbert E. et al. Preceptorship
Program on IUC insertion - Modules 2 and 4.
The uterus should measure between 6 and 10 cm with a sound. If the sound does not advance past 4 cm, you are likely in the cervix. If the sound passes beyond 10 cm or has no resistance, consider perforation and STOP.
Costescu et al. Levonorgestrel-Releasing Intrauterine Systems for Long-Acting Contraception: Current Perspectives, Safety, and Patient Counseling.Int J Womens Health 2016.
Prior to placement, the uterine cavity should be measured, either with a metal or plastic sound, or a disposable hysterometer. This ensures the uterine cavity is the appropriate size for an IUD, informs the clinician as to the depth the device should be placed, confirms that it will be possible to pass through the internal cervical os, and forewarns a woman as to the sensation that will be felt during device placement.
7 Steps to sounding the uterus as described in the IUD Guidelines for Family Planning Service Programs: A Problem-Solving Reference Manual
If the cervix does not sound beyond 4 cm:
Warning signs of perforation:
Warning signs of a false passage:
If there is concern for perforation or a false passage, STOP.
Costescu D. and Guilbert E. et al. Preceptorship Program - Modules 3 and 4
Infections related to IUC placement are rare, and usually related to preexisting infection. Universal screening does not reduce the risk of PID compared to screening based on risk factors.
Women at elevated risk of STI (non-monogamous, history of STI, 25 or younger) should be screened at the time of placement. Universal STI screening does not reduce the risk of PID.
An IUC should not be placed if there is mucopurulent discharge, or if there is a known positive swab, until treatment is completed.
While bacterial vaginosis may increase the risk of infection, routine screening for BV at the time of placement is not recommended. If there is clinical suspicion of BV, it may be treated at the time of placement.
Costescu D. and Guilbert E. et al. Preceptorship
Program - Module 3
SOGC Clinical Practice Guideline, Canadian Contraception
Consensus (part 3): Chapter 7 – Intrauterine Contraception
The cervix should be stabilized with a tenaculum prior to device placement. This is to straighten the axis of the uterus (from an anteverted or retroverted position) and make placement easier and possibly less painful. It may also reduce the risk of perforation as a steeply angled uterine cavity may increase the risk of perforation.
While a tenaculum looks intimidating, placement is relatively painless. Having a woman cough upon tenaculum placement reduces pain. Alternatively, some clinicians use a small atraumatic clamp, instead.
Costescu D. and Guilbert E. et al. Preceptorship Program - Module 3
Following placement of a device, a woman should come back for
follow-up in 4-12 weeks to assess satisfaction, review side
effects, and, if needed, perform a string check.
Following an uncomplicated placement, an ultrasound is
not necessary.
An ultrasound should be considered if:
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception
Unscheduled bleeding with a Copper IUD is relatively common, and will often improve with time. It is normal for women to experience spotting following placement of a Copper IUD, particularly when placement occurs in the luteal phase. It usually abates with time, however ongoing unscheduled bleeding at 6 months is unlikely to spontaneously resolve.
When a woman with previously normal bleeding experiences new unscheduled bleeding, a reassessment should take place, including confirmation of correct device placement and STI swabs.
A trial of combined hormonal contraception may be considered to see if unscheduled bleeding abates with time. For women who like using an IUD but require menstrual management, a LNG-20 should be considered, although a lower-dose device may still provide a decrease in dysmenorrhea and flow.
Unscheduled bleeding and spotting is common following LNG-IUS placement, and will often improve with time. In general, after 6 months of use, unscheduled bleeding is unlikely to abate.
While multiple treatment modalities have been studied, none has provided conclusive benefit. Appropriate first-line options include NSAIDS, tranexamic acid, combined hormonal contraception, and low-dose doxycycline (40-50 mg daily), or empiric treatment of doxycycline (100 mg BID for 10 days).
While it has been conventionally taught that “once amenorrhea occurs it will stay”, it may be normal for women who have experienced amenorrhea from an LNG-IUS in one 12 month period to experience some bleeding in another 12 month period. This phenomenon has been observed in clinical trials of a new 52mg LNG-IUS, which is approved in other countries.
When a woman who has previously enjoyed a favourable menstrual pattern with an LNG-IUS experiences a return of problematic bleeding in the 4th year of use or beyond, the device should be replaced. If bleeding recurs in years 2 or 3, it may be advisable to first rule out other causes, such as a polyp or cervicitis.
While multiple treatment modalities have been studied, none has provided conclusive benefit. Appropriate first-line options include NSAIDS, tranexamic acid, combined hormonal contraception, low-dose doxycycline (40-50 mg daily), or empiric treatment with doxycycline (100 mg BID for 7-10 days).
More information on Managing Breakthrough Bleeding
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception Expert consensus (CNIC)
As women approach the end of their reproductive years, they may develop risk factors or medical conditions for which estrogen containing contraceptives are contraindicated, such as hypertension. Additionally, age may add sufficient risk to preexisting conditions (such as smoking) to preclude the safe use of some methods.
As estrogen-free options, IUCs are usually safe for women during the menopause transition. Copper IUDs should be left in situ until amenorrhea occurs for one year, at which point they can be removed. LNG-IUS users may wish to have the device removed at 55, or when FSH testing confirms that menopause is likely (>35U/L).
The LNG-20 is approved in some countries (not Canada) for endometrial protection during Menopausal Hormone Therapy (HT). A woman receiving HT does not need additional progesterone if an LNG-IUS is in situ. Similarly, an LNG-IUS can be considered in a woman who requires endometrial protection and wishes to minimize her exposure to hormones.
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception
A vasovagal reaction is a self-limiting period of bradycardia and hypotension, related to cervical excitation. Rarely, it can occur following placement.
Costescu D. and Guilbert E. et al. Preceptorship Program on IUC insertion - Module 4
IUCs do not increase the risk of thrombosis. A copper IUD has no impact on hemostatic parameters and does not increase the risk of VTE. However, a copper device should be used with caution in women who are currently using anticoagulants (for example, because of a history of VTE or thrombophilia) since there is a potential for increased menstrual blood loss.
In several cohort studies, the risk of VTE among LNG-IUS users is at or below population baseline. They can be used safely in women with a history of VTE or inherited thrombophilia, and the menstrual benefits may be useful among women on anticoagulation therapy.
SOGC Clinical Practice Guideline, Canadian Contraception Consensus (part 3): Chapter 7 – Intrauterine Contraception
Multiple studies confirm that neither copper IUDs or progestin IUS’ are associated with weight gain. Some women experience mild breast tenderness and bloating sensation with a progestin IUS, which will decrease over the first 3 months. This is self-limiting and does not constitute weight gain.
Women who are worried about weight gain should be weighed at the consultation, placement, and follow-up visits.
Black D. and Waddington A. et al. Build Your Expertise: IUC slide deck:39-41.