
Home
Asking the woman to cough while you place the tenaculum on the anterior lip of the cervix can help reduce discomfort with this aspect of the procedure. Warming the speculum and/or gel can also add to a more pleasant start to the placement procedure.
Costescu et al. Levonorgestrel-Releasing Intrauterine
Systems for Long-Acting Contraception: Current Perspectives,
Safety, and Patient Counseling.Int J Womens Health 2016.
Black D. and Waddington A. et al. Build Your Expertise: IUC
slide deck: 34.
Costescu D. and Guilbert E. et al. Preceptorship Program on
IUC insertion - Modules 3 and 4.
SOGC Clinical Practice Guideline, Canadian Contraception Consensus
(part 3): Chapter 7 – Intrauterine Contraception
Waddington A. and Reid R. More harm than good: the lack of
evidence for administering misoprostol prior to IUD insertion.
JOGC
2012;34(12):1177-79.

Allow women to use their smartphones (without recording) during the placement – often checking social media or playing an addictive game helps provide a distraction. Alternatively, an interesting “seek and find” poster in the examination room provides distraction during placement
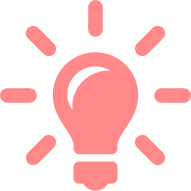
Misoprostol Is not recommenced prior to IUC placement
Several studies report no benefit from misoprostol (Prostaglandin E1). An RCT of 270 women having a copper IUD or LNG-20 placement compared 400 ug misoprostol PV vs. placebo, three hours before placement. The very finding were:
In addition to good technique (reassurance, slow placement, cough distraction, and avoiding excessive application of the tenaculum beyond the first ratchet “click”), local application of anaesthetic may reduce pain of IUS placement.
An RCT among 74 women compared an injection of 2 mL xylocaine 1% at 12 o’clock versus an application of 1 mL xylocaine gel 2% on the anterior lip before IUC placement. Pain scores are lower with injection of xylocaine.
When injecting xylocaine in the cervix, bleeding and extrusion of the anaestetic may occur. Direct pressure, with either a cotton-tip swab or clamp for 1 minute will stop bleeding and allow the anaesthetic to work.
Inject 5 mL at each 4 and 8 o’clock, towards the uterosacral ligaments, infiltrating deep into the tissue.
Please note that the placement of the cervical block itself can be painful and, as such, it should not be routinely performed.
If a woman with an IUC in place more than 6 months, or following a period of being pain-free, develops new severe cramping or abdominal tenderness, one must rule out: