Perforation
STOP, Stabilize, and Scan
Perforation is a rare complication of IUC placement, and occurs in
one in a 700-1000 placements. Recognizing perforation at the time
of placement reduces the risk of inadvertent migration or
intraabdominal placement of a device.
Symptoms of perforation:
- Excessive pain
- Sudden loss of resistance
- Excessive measurement with sound or IUC insertion tube
-
IUC inserter does not follow expected path of uterine axis
-
Do not continue with IUC placement if a sound has perforated the
uterus
Most are fundal perforations and require no further management.
-
Monitor the woman:
-
Vital signs including blood pressure, oxygen saturation,
abdominal exam and bimanual examination to assess pain and
bleeding.
- Consider CBC if concerned about hemodynamic status.
- Ultrasound as clinically indicated.
-
If the woman is stable: inform her of signs and symptoms to
observe and let her go home.
-
If the woman is unstable, initiate resuscitation and obtain
an emergent gynaecology consultation.
-
Women with vaso-vagal reactions may look unstable, but the
symptoms are usually self-limiting.
-
If an IUC is found to be placed in the abdomen (a very rare
event), refer to gynecologist. Laparoscopic surgery may be
required.
Costescu D. and Guilbert E. et al. Preceptorship Program -
Module 4
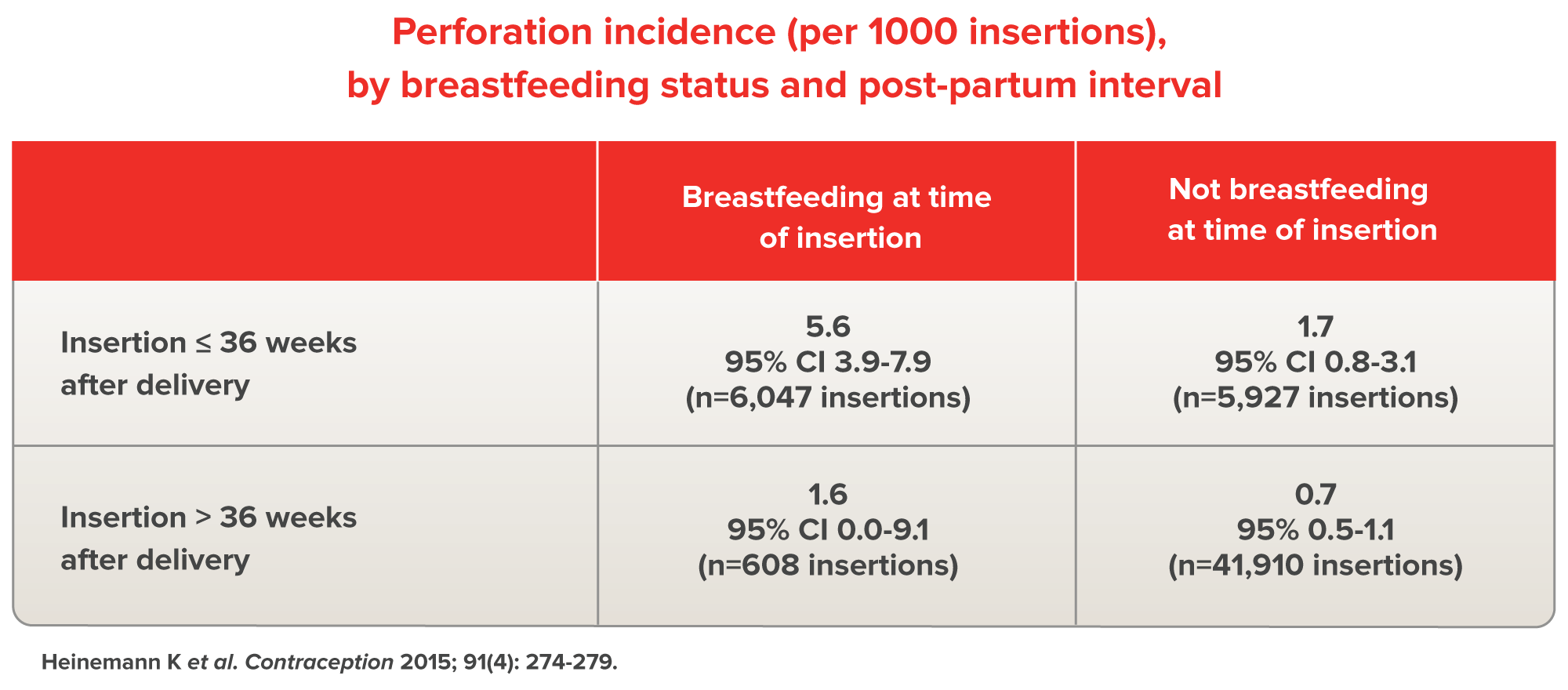
Heinemann K et al. Risk of uterine perforation with
levonorgestrel-releasing and copper intrauterine devices in the
European Active Surveillance Study on Intrauterine Devices.
Contraception 2015; 91(4): 274-279.
Perforation Incidence
The EURAS-IUD (European Active Surveillance Study for
Intrauterine Devices) was a large, prospective, comparative,
non-interventional, cohort study (n = 61,448) in parous women
using LNG-20 (Mirena) and copper IUD the incidence of
perforation was 1.3 (95% CI: 1.1 - 1.6) per 1000 insertions in
1 year.
Specifically:
-
61 perforations occurred for LNG-IUS (n=43,078; 1.4 per
1,000 insertions; 95% CI: 1.1-1.8)
-
20 for copper IUDs (n=18,370; 1.1 per 1,000 insertions; 95%
CI: 0.7-1.7)
-
Current breastfeeding and postpartum insertion up to 36
weeks were associated with increased risk of perforation
-
There were no serious complications in any of the women who
experienced a perforation, nor in any woman who required
laparoscopic removal.
Risk Factors for Perforation
Certain clinical scenarios increase the risk of perforation.
While in most cases this should not preclude an attempt at IUC
placement, some clinicians will prefer to refer to a more
experienced provider.
Risk Factors for Uterine Perforation
- Postpartum state
- Breastfeeding
- Grand multiparity
-
Lack experience of health care professional (HCP) performing
placement
- Fixed and/or retroverted uterus
- Uterine anomaly
Nulliparous women are not at increased risk of
perforation.
In a large post-marketing study, no difference between the
rates of perforation in nulliparous and multiparous women was
observed. This is also true for mode of delivery (caesarean
vs. vaginal).
Recognizing Perforation at Follow-up
Partial perforation (uterine embedment) or complete
perforation of the uterine wall or cervix may occur during or
following placement. The vast majority of perforations occur
at the time of placement, though it may not be detected. As
such, a follow-up visit is important. A delay in detection may
result in a partially perforated IUC migrating to a complete
perforation (a missed opportunity to remove the IUC in the
office before a complication arose), increased risk of
laparoscopic removal, and, very rarely, intraabdominal injury.
Thankfully, the risk of major complication following IUC
placement, even in the setting of perforation, is very rare. A
woman should be informed of the small risk of perforation, and
the importance of prompt diagnosis.
-
Women with an embedded device or unrecognised perforation
may present with:
-
Persistent abnormal bleeding and/or abdominal pain
-
Acute episodes of pelvic pain (often unilateral), which
can be provoked with intercourse. Typically, a
correctly-placed IUC does not cause dyspareunia.
- Asymptomatic or incidental ultrasound findings
- Shortened or missing IUC strings
- Pregnancy
- Difficult removal attempt
- Some are asymptomatic
-
This may decrease contraceptive effectiveness and result in
pregnancy, especially for Cu IUDs. Some women with a
migrated IUS will remain amenorrheic.
-
Usually diagnosed by ultrasound, although x-ray or CT scan
can be useful adjuncts. MRI is not ideal as the IUD may
affect image quality.
-
An embedded or perforated device should be removed on a
semi-urgent basis.
-
For an embedded device, an office removal with or
without paracervical block may be sufficient.
-
An examination under anaesthesia, hysteroscopy, and/or
curettage may be needed for a difficult removal.
-
For an intraabdominal device, operative laparoscopy is
the preferred approach. Most often, the device is in the
posterior cul de sac, or adherent to the omentum. As a
result, the IUC may be located in the upper abdomen
during a laparoscopy (as the omentum is moved superiorly
to visualize the pelvis)