
Home
Start by asking the woman if her current method meets these needs, and if she would like to learn about other options.
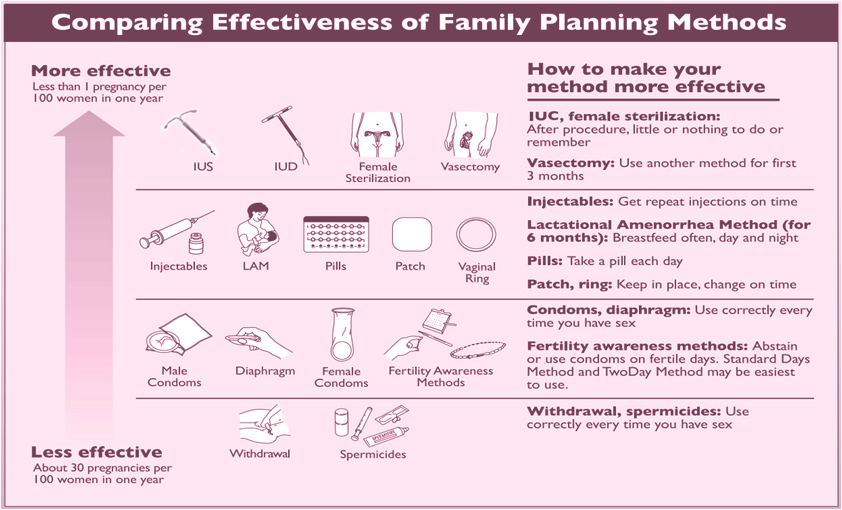
WHO depiction of contraceptive choices, stratified by
effectiveness:
Intrauterine contraception, a Long-Acting Reversible Contraceptive
(LARC) Method, is a top tier method. The commonly used “Pill,
Patch, Ring” (PPR) methods are considered “second tier”.
SOGC Clinical Practice Guideline, Canadian Contraception Consensus
(part 3): Chapter 7 – Intrauterine Contraception Initiative of the
SOGC www.sexandu.ca Black D.
and Waddington A. et al. Build Your Expertise: IUC slide
deck: 35,46,50-52,78.
Costescu D. and Guilbert E. et al. Preceptorship Program on
IUC insertion - Module 2 SOGC - Postpartum contraception slide
deck
Finding the Right Match
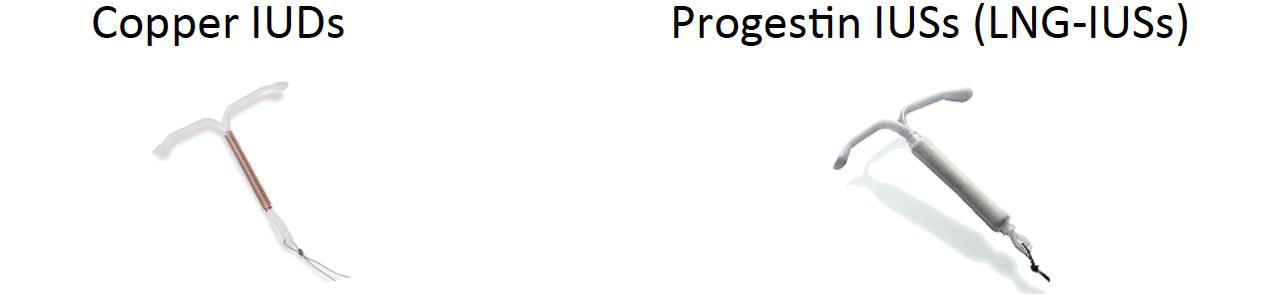
Long Acting Reversible Contraception (LARC, or sometimes called long-acting contraception-LAC) requires administration less than once per year. In Canada, Intrauterine Contraception (IUC), which consists of Copper Intrauterine Devices (Cu-IUD) and Levonorgestrel-Releasing Intrauterine Systems (LNG-IUS), is the only LARC method available to women.
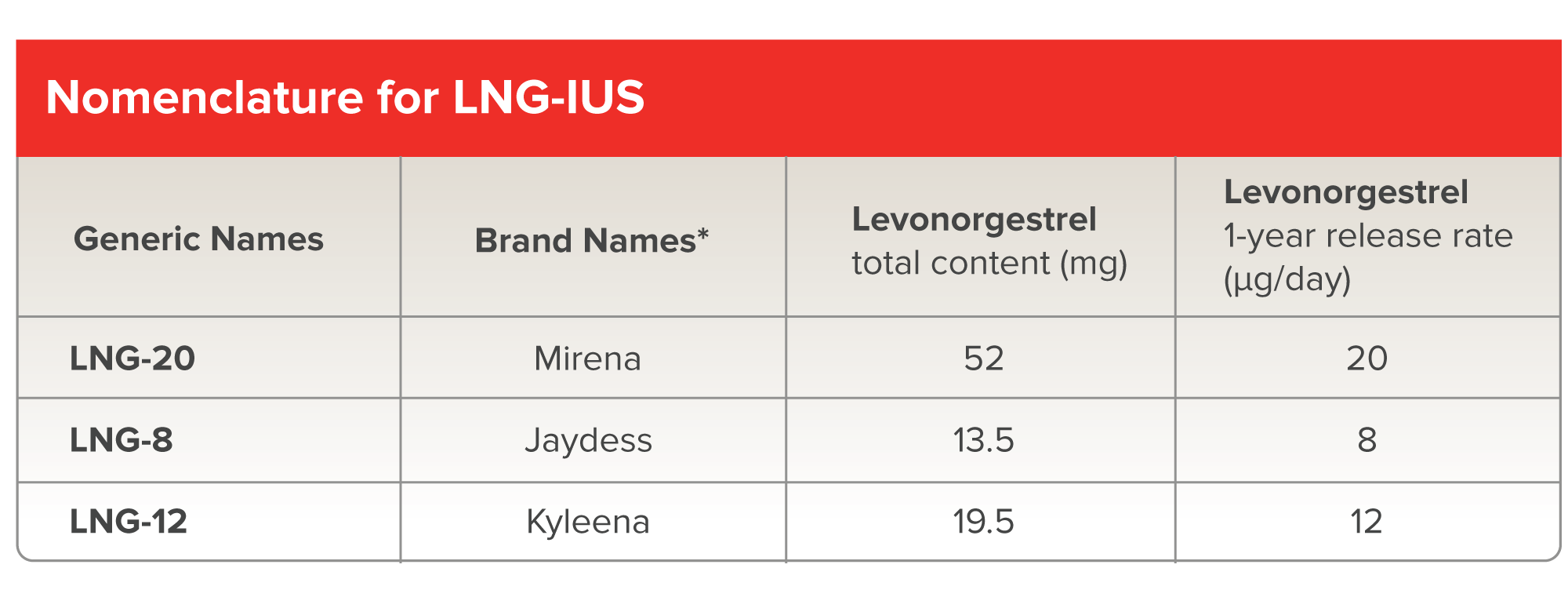
IUCs are a form of LARC that is placed into the uterus. Two categories of IUC are available in Canada: the copper IUD (Cu-IUD) and levonorgestrel-releasing intrauterine systems (LNG-IUS).
The US Medical Eligibility Criteria for Contraceptive Use provides guidance on the use of the various contraceptive methods given a medical condition. To learn more, click here